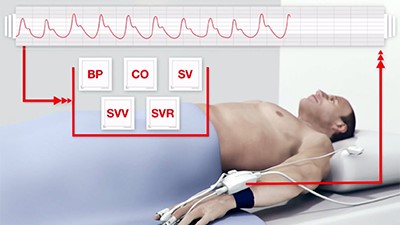
Advanced hemodynamic monitors and fluid responsiveness
Cardiac output is used in the ICU as a marker of oxygen delivery to tissues and to guide treatment, primarily for fluid resuscitation and the use of vasopressors, vasodilators and inotropes.
For decades, PA catheter used to be the ‘clinical reference standard’ for cardiac output monitoring, using thermodilution technique. However, after PAC-MAN study, PA catheters were shown to have no mortality benefit and since then, it’s use has declined considerably. Despite this, the PA catheter is still considered the gold standard for cardiac output measurement, against which all new monitors are measured.
In recent times, there was a development of number of less invasive techniques to measure cardiac output that require A-line (PiCCO, LiDCO, Vigileo) or central line (PiCCO, LiDCO). Other available non-invasive techniques for continuous CO monitoring also includes esophageal Doppler, partial CO2 rebreathing, bioimpedance, bioreactance and volume clamping.
Where can we use:
Although the non-invasive techniques show reasonably good results in elective postoperative ICU patients, the noninvasive techniques are not able to replace PA catheter for accurate cardiac output measurements in non-elective ICU patients. Overall the non-invasive techniques seem to perform more as a trend monitoring device rather than measuring absolute cardiac output.
Minimally invasive cardiac output monitors
Pulse contour analysis (FloTrac/Vigileo, PiCCO, Volume View and LiDCO monitor):
It was based on the premise that cardiac output is directly proportional to pulse pressure. In fact, pulse pressure is considered to be poor man’s stroke volume. Pulse contour devices use the same principle and relate the contour of the arterial pressure waveform to stroke volume and SVR. A proprietary algorithm is used to determine the cardiac output.
Cardiac output monitoring utilizing pulse contour analysis is one of the most extensively studied of all the minimally invasive monitoring systems. In general, they all show good agreement with cardiac output measurements made using a PAC. Despite this, we should be aware of a number of sources of potential error, which may be more pronounced in some clinical settings.
Limitations: They rely on an optimal arterial signal. Over or under-damped traces may lead to inaccurate cardiac output measurement. Arrhythmias, aortic regurgitation, and the use of IABP all affect pulse contour, leading to inaccurate readings. Changes in SVR will also lead to inaccuracies in cardiac output measurement.
They also provide stroke volume variation (SVV) with respiration as an indicator of fluid responsiveness. SVV is the difference between maximum and minimum stroke volumes over the respiratory cycle and is caused by changes in preload with alterations in intra-thoracic pressure. In general, SVV > 15% or greater are presumed to be fluid responsive.
FloTrac/Vigileo
It is based on the principle that aortic pulse pressure is proportional to stroke volume (SV) and inversely related to aortic compliance. Cardiac output is calculated every 20 s using a proprietary algorithm.
The first step in this monitor is to calculate pulse pressure using the arterial wave form. It uses a proprietary constant called Khi. Khi is a multivariate polynomial equation which assesses the impact of the patient’s ever-changing vascular tone on pulse pressure. Khi is calculated by analyzing the patient’s pulse rate, MAP, standard deviation of MAP, large vessel compliance as estimated by patient demographics, and skewness and kurtosis of the arterial waveform. Khi is updated and applied to the FloTrac system algorithm every minute. Then, stroke volume is calculated, which is a product of pulse pressure x Khi value. The rest of the variables including CO, SVV and SVR are all derived from the stroke volume.
Unlike other pulse contour devices, the FloTrac/Vigileo does not require external calibration. However, it is less accurate for absolute measurement than calibrated pulse wave devices.
Limitations:
Stroke volume variation has the following limitations
-
Mechanical ventilation: Currently, literature supports the use of SVV on patients who are 100% mechanically (control mode) ventilated and fixed respiratory rates.
-
No Spontaneous breathing: Currently, literature does not support the use of SVV with patients who are spontaneously breathing.
-
Tidal volumes at least 8cc/kg
-
No arrhythmias: SVV is unreliable in presence of arrhythmias.
Other considerations, which could potentially limit the reliability of FloTrac are:
-
Heart rate (HR) >150 beats per minute
-
Heart rate to respiratory rate ratio < 3:1
-
Respiratory rate > 35
-
Open chest
-
Right ventricular failure
-
Pneumoperitoneum
-
Poor arterial waveform
-
Raised intra-abdominal pressure
-
Raised intra-thoracic pressure
-
An open abdomen has been shown to reduce SVV by 40-50%
-
Decreased lung compliance and pulmonary hypertension may diminish SVV and PPV as predictors of fluid responsiveness.
-
Decreased extra pulmonary compliance ( obesity, ascites, pleural effusion, chest wall edema)
-
High levels of PEEP can increase SVV
-
Vasodilatory drugs can increase SVV
Accuracy: It was not very accurate in tracking changes of cardiac output, induced by norepinephrine. Br J Anaesth. 2012 Apr;108(4):615-22. In one of the studies comparing it to PA catheter, FloTrac underestimated cardiac output by more than 2 L in 41% of the patients. Br J Anaesth. 2011 May;106(5):690-4. Also, at high cardiac output levels, it frequently underestimates PAC measurements and it is not as reliable as thermodilution in hyperdynamic liver transplant patients. J Cardiothorac Vasc Anesth. 2008 Oct;22(5):681-7.
PICCO and Transpulmonary thermodilution:
It uses an A- line to measure the aortic waveform and uses its algorithm to determine the cardiac output by integrating the area under the curve of the arterial pressure vs time trace. A central venous catheter (CVC) is used to calibrate the system using a transpulmonary thermodilution technique.
The cold injectate is introduced into the SVC via a central line. An A- line with a thermistor is placed in a major artery (femoral, axillary, or brachial) and the change in temperature of the blood is measured after the injectate has traversed the right heart, pulmonary circulation, and left heart. The thermodilution equation is used to calculate the cardiac output.
Accuracy: In the study on liver transplant patients, pulse contour analysis was very inaccurate compared to PA catheter, more so when patients are on vasopressors. Transplant Proc. 2003 Aug;35(5):1920-2
Volume View and Transpulmonary thermodilution:
It uses the same transpulmonary thermodilution concepts to measure key elements of oxygen delivery such as cardiac output and volumetric variables to assess components of cardiac output such as preload and contractility. In addition, lung water measurements are available that can assist the clinician in treating patients with lung injury and cardiac failure.
Transpulmonary thermodilution cardiac output uses the same principles as right heart thermodilution except the thermal bolus is injected into the central venous system and moves across the right heart, lungs, left heart and out into the arterial tree where the thermal change is measured over time by an embedded thermistor on a catheter inserted into the femoral artery.
Volume View measures
-
Intermittent transpulmonary thermodilution cardiac output
-
Calibrated continuous cardiac output
-
Intermittent or continuous SVR
-
Global End Diastolic Volume
-
Global Ejection Fraction
-
Extra-Vascular Lung Water index
-
Pulmonary Vascular Permeability Index
Global end diastolic volume – GEDV is closely related to the volume within all four chambers at the end of diastole. It can be used to assess preload and manage a patient’s volume resuscitation. The rate of change of upslope and downslope of the thermodilution waveform is used to calculate GEDV.
Global Ejection Fraction – GEF can be used to assess global cardiac function.
-
Cardiac Output / Pulse Rate = Stroke Volume
-
Stroke Volume * 4 / GEDV = Global Ejection Fraction
-
Global Ejection Fraction normal range is between 25-35%
Extra Vascular Lung Water index: EVLW can be used to assess the level of pulmonary edema which may be the result of heart failure, volume overload, or lung injury and can interfere with the ability of the lungs to oxygenate the blood. This is indexed against the patient’s predicted body weight to obtain Extra Vascular Lung Water Index or EVLWI. The “normal” value for EVLWI is reported to be 3–7 mL/kg. Values above 10 mL/kg indicate pulmonary edema and values as high as 15-20 ml/kg indicate severe pulmonary edema.
Pulmonary vascular permeability index: PVPI is calculated by dividing extra vascular lung water by pulmonary blood volume. PVPI is increased (> 3) in patients with increased pulmonary permeability due to lung injury and normal in patients with hydrostatic and cardiogenic pulmonary edema.
LiDCO and Pulse power Analysis
It uses pulse power analysis rather than pulse contour analysis. It uses an algorithm based on the law of conservation of mass for continuous cardiac output calculation. By assuming that net power has a linear relationship with net flow, an algorithm is used to calculate cardiac output. A standard A- line is required and it can be calibrated using lithium dilution (either central line or peripheral IV).
The lithium is injected via a central or peripheral venous line and measured via aspiration of blood through an arterial catheter, with an attached disposable electrode selective for lithium, at a constant rate of 4 ml/min.
Accuracy: The LiDCO pulse pressure device correlates well with the PA catheter, even in patients with hyperdynamic circulation. Intensive Care Med. 2008 Feb;34(2):257-63.
Noninvasive hemodynamic monitors
-
Esophageal Doppler
-
Transthoracic doppler
-
Partial CO2 rebreathing
-
Bioimpedance
-
Bioreactance
-
Volume clamping
-
Transthoracic ECHO
Esophageal Doppler (Cardio Q)
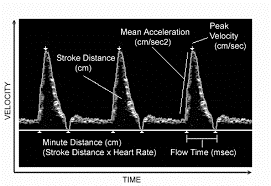
A flexible probe with a Doppler transducer at the tip of the probe is inserted orally or nasally into the esophagus and the transducer is positioned facing the descending aorta. The CardioQ monitor displays a waveform and stroke volume is calculated using that waveform.
Advantages: It can be placed easily.
Limitations: Since the probe is placed in the descending aorta, the doppler approach cannot directly measure CO and relies on the assumption of a fixed relation where 30% of CO is diverted proximally to the descending aorta. Moreover, the CardioQ may not be reliable in situations such as severe aortic stenosis, because of turbulent blood flow. The technique is operator dependent and incorrect placement of the probe can alter the CO measurement.
Accuracy: The esophageal Doppler monitor has high validity (no bias and high clinical agreement with pulmonary artery thermodilution) for monitoring trends in cardiac output (5 studies, clinical agreement of 86%). However, it is not so good in measuring absolute cardiac output estimation (16 studies, clinical agreement 52%). Intensive Care Med. 2004 Nov;30(11):2060-6.
Aortic Doppler (USCOM)
Cardiac output can be estimated using doppler ultrasound to determine the flow of blood through the aorta. It uses a transthoracic doppler probe placed suprasternally to measure flow through aorta or on the left side of the chest to measure transpulmonary flow.
The velocity–time integral (VTI) is calculated from the area under the velocity–time curve and used as the stroke distance. It then uses a nomogram for aortic cross-sectional area estimation or use an M-mode. Cardiac output is then calculated using the equation:
CO x Aortic cross sectional area x HR= Cardiac output.
Finally, a correction factor must be used as the measurement utilizes the descending aorta, as only 70% of cardiac output passes through this vessel.
Advantages: It can be placed easily.
Limitations: The use of a nomogram to estimate of aortic cross-sectional area is very error prone, especially as aortic valve area will change with change in vascular tone and volume status. The probe position is critical in reducing error for both blood flow measurement and aortic cross sectional area. Even small misalignments of the ultrasound beam with blood flow will lead to underestimation of flow and cardiac output. Also, it is not so accurate with aortic stenosis.
Accuracy: The USCOM device has shown variable results, especially in low and high cardiac output states. Emerg Med Australas. 2008 Jun;20(3):201-8
Partial carbon dioxide (CO2) rebreathing (NICO monitor)
The partial CO2 rebreathing method uses Fick’s principle applied to CO2 elimination. A rebreathing apparatus is attached to the patient’s ET tube and serial measurements are taken every 3 min. At steady state, the amount of CO2 entering the lungs via the pulmonary artery is proportional to the cardiac output and equals the amount exiting the lungs via expiration and pulmonary veins. During 30 s of rebreathing, the amount entering does not change, but the amount eliminated by expiration decreases and the EtCO2 increases in proportion to the cardiac output.
The computer cycles every three minutes from the non-rebreathing mode to a 30-second period of rebreathing by adding an additional dead space with a disposable rebreathing loop.
The calculation of CO by the NICO monitor only reflects part of the pulmonary capillary blood flow that participates in the gas exchange. It might have some limitations in conditions like ARDS which has very poor gas exchange. NICO system claims that it includes a correction for the amount of shunted blood, based on FiO2 and SaO2.
Advantages: Easy use and does not require A-line or central line.
Limitations: This technique is restricted to the mechanically ventilated patient. Because of the non-rebreathing and rebreathing cycle, it has a relatively long response time, making it less useful for continuous cardiac output monitoring. It also will not give stroke volume variation.
Accuracy: When compared with the PA catheter, it could have an error rate of up to 45%. Its accuracy is improved when patient is hemodynamic stable, on controlled mechanical ventilation without overt pulmonary disease. It is less accurate when there is more than 10% variability in tidal volumes and hence is inaccurate in patients on assisted spontaneous breathing. Severe chest trauma, significant intrapulmonary shunt, low minute ventilation, and high cardiac output may all reduce accuracy.
Bioimpedance
It is based on the theory that with every heart beat the electrical resistance (impedance) of the thorax changes, because of a shift in intrathoracic blood volume. Impedance cardiography relies on measured changes in signal amplitude of a transmitted electrical current via four electrodes placed on the neck and thorax. Then it uses proprietary algorithm to derive the stroke volume.
Advantages: Easy use and does not require A-line, central line or ventilator.
Limitations: Operator error can occur with the incorrect placement of the sensors. Moreover, bioimpedance is sensitive to ambient electrical noise and patient movement. Pulmonary edema, pleural effusion, hyperventilation, high levels of PEEP, chest tubes and variations in patient body size and skin humidity can interfere with the electrical conductivity and therefore make CO measurements inaccurate. Arrhythmias can affect the cardiac output measurement as well.
Accuracy: Overall, bioimpedance seems an unreliable method for absolute CO measurement in the ICU, since it is affected by so many variables.
Bio reactance (NICOM monitor):
It is based on analysis of relative phase shifts of a high-frequency current, applied across the thorax and recorded from the left and right side of the thorax, by four dual electrodes placed at the corners of the thorax. These relative phase shifts are related to changes in intrathoracic blood volume, so that the peak rate of change in the relative phase shift is related to the peak aortic flow during a heartbeat.

Advantages: It is easy to use and interpret and can be used in conscious as well as unconscious patients. Also, bio reactance is not based on changes in amplitude-like bio impedance, and hence, it is less limited by factors such as body size, pleural and pulmonary fluid and patient movement.
Limitations: Theoretically, as with bioimpedance, bio reactance will overestimate the CO in patients with aortic insufficiency. Moreover, measurements can be altered by nurse’s interventions, movements of the patient or loss of patch adhesive which occur over time.
Accuracy: Validation studies have shown good agreement between bio reactance and PA catheter in measuring CO, in postoperative cardiac surgery patients, in awake surgical and non-surgical ICU patients and patients with pulmonary hypertension. However, most of these studies were funded by NICOM manufacturing company.
In one unfunded study, NICOM did not accurately estimate the cardiac output in critically ill patients. Moreover, it could not predict fluid responsiveness through the PLR test. Br J Anaesth. 2013 Dec;111(6):961-6
As bio reactance shows similarities with the bio impedance technique we should bear in mind that future studies might show data containing more negative results.
Volume clamping (ClearSight)
The device works by combining continuous finger blood pressure measurement via the volume clamp method, brachial pressure reconstruction and the pulse contour method.
Continuous finger blood pressure measurement is established by wrapping the cuff around the middle phalanx of a finger. The pressure controller continually adjusts the pressure in the finger cuff’s inflatable bladder with the result that the arteries and bladder are equal in pressure and the arteries no longer pulsate. The volume of the arteries at this point is referred to as the unloaded volume. The pressure that is required to continuously maintain the unloaded volume is equal to the blood pressure in the finger.
Brachial wave reconstruction: Since the arteries narrow as the distance from the heart increases, increased resistance and backwards reflection of the pressure waves occurs. This results in varying pressure levels and waveform shapes. The finger site has slightly lower mean pressure levels and a higher peaked waveform. The brachial pressure waveform is modified from the finger pressure waveform by an algorithm. Finally, the pulse contour method is used to estimate CO from the arterial waveform.
The first step in this monitor is to calculate finger blood pressure using the arterial wave form. Then, afterload is estimated from its algorithm using patient’s demographics and arterial compliance.
Advantages: It is easy to use and interpret and can be used in conscious as well as unconscious patients.
Limitations: The system is not suitable in patients with severe peripheral vasoconstriction, very edematous fingers, aortic regurgitation and ascending aortic aneurysm.
Accuracy: When compared to PA catheter, ClearSight seems to be less accurate in patients with a low cardiac output. However, in most patients, ClearSight is able to track hemodynamic changes induced by a fluid challenge or passive leg raising test. Curr Opin Crit Care. 2015 Jun;21(3):232-9.
Most of the other studies also reported a high percentage error (average of 44%). In general, ClearSight showed the same trend in cardiac output as PA catheter but when looking not only at the trend but also the absolute value of cardiac output, the results are conflicting (concordance between 94% and 100% but correlation coefficients between 0.39 and 0.94). Since the fixed algorithm incorporated to calculate CO depends on assumptions, the reliability of ClearSight might alter in different patient groups or clinical scenarios.
On their own website, cardiac output measurement has an error rate as high as 57%.
Cardiac output validation studies
|
Vs. Pulmonary thermodilution
|
Patients
|
Percentage Error
|
|---|---|---|
|
Bubenek-Turconi – Anesth & Analg 2013 39
|
25 post CABG patients
|
39%
|
|
Bogert et al – Anaesthesia 2010 40
|
25 post CABG patients
|
30%
|
|
Stover et al – BMC Anesthesiology 2009 41
|
10 severely ill ICU patients
|
29%
|
|
Vs. Transpulmonary thermodilution
|
|
|
|
Broch et al – Anaesthesia 2012 42
|
40 cardiac surgery patients
|
23%/26%
|
|
Monnet et al – Critical Care 2012 43
|
45 severely ill ICU patients
|
57%
|
|
Vs. Trans-thoracic echo-Doppler
|
|
|
|
Van der Spoel et al. – J Clin Anesth 2012 44
|
40 ASA 1&2 patients
|
39%
|
|
Van Geldorp et al. – Europace 2011 45
|
23 CRT patients
|
15%
|
|
Vs. Esophageal echo-Doppler
|
|
|
|
Chen et al. J Clin Anesth 2012 46
|
23 ASA 1-3 patients
|
37%
|
My final verdict: In elective postoperative ICU patients, with stable tidal volumes and without pulmonary disease, the techniques have shown reasonably good results. In non-elective ICU patients, however, the non-invasive techniques are not able to replace PA catheter, mostly because of underlying diseases which can interfere with the accuracy.
In a nut shell, noninvasive techniques are less effective in measuring absolute CO compared with PA catheter. However, they can be used as CO trend monitors in elective postoperative ICU patients. In my personal opinion, they should rarely be used in ICU population who usually has complex disease processes.
References: