Basic Life Support (BLS)
Immediate recognition and activation, early CPR, and rapid defibrillation (when appropriate) are the first three BLS links in the adult Chain of Survival. Patient survival depends primarily upon immediate initiation of excellent CPR and early defibrillation. AHA Guidelines 2015

Chest compressions
Chest compressions are the most important element of cardiopulmonary resuscitation (CPR). The recommended sequence for a single rescuer is to initiate chest compressions before giving rescue breaths (C-A-B rather than A-B-C) to reduce delay to first compression. The single rescuer should begin CPR with 30 chest compressions followed by 2 breaths. Coronary perfusion pressure and return of spontaneous circulation (ROSC) are maximized when excellent chest compressions are performed. The mantra of the AHA BLS Guidelines is: "push hard and push fast on the center of the chest”.
The following goals are essential for performing excellent chest compressions:
-
Maintain a rate of at least 100-120 compressions per minute
-
Compress the chest at least 2 inches with each down-stroke, but not greater than 2.4 inch.
-
Allow the chest to recoil completely after each down-stroke (eg: it should be easy to pull a piece of paper from between the rescuer’s hand and the patient’s chest just before the next down-stroke)
-
Minimize the frequency and duration of any interruptions
When preparing for defibrillation, rescuers should continue performing excellent chest compressions while charging the defibrillator until just before the single shock is delivered, and resume immediately after shock delivery without taking time to assess pulse or breathing. No more than three to five seconds should elapse between stopping chest compressions and shock delivery.
Note: Never hold compressions for putting central lines, ECHO, intubation or any other procedures except for defibrillation. ONLY CPR AND SHOCK IS PROVEN TO BE HELPFUL. Even ACLS says that drugs like Epinephrine may or may not be helpful. Multiple studies showed that CPR only resuscitation is equally good as chest compressions with rescue breathing. N Engl J Med. 2000 May 25;342(21):1546-53 , N Engl J Med. 2010 Jul 29;363(5):423-33 , N Engl J Med. 2010 Jul 29;363(5):434-42
Ventilation
Patients are often over-ventilated during resuscitations, which can compromise venous return, because of positive intrathoracic pressure during ventilation, resulting in reduced cardiac output and inadequate cerebral and cardiac perfusion. Proper ventilation for adults includes the following:
-
Give 2 ventilations after every 30 compressions for patients without an advanced airway
-
Give each ventilation over no more than one second
-
Provide enough tidal volume to see the chest rise
-
Avoid excessive ventilation
-
Give 1 asynchronous ventilation every 6 seconds (10 per minute) to patients with an advanced airway (eg, supraglottic device, endotracheal tube) in place
-
Do not hyperventilate even if there is significant acidosis because of risk of decreasing cardiac output. Infact, everybody who is coding will have lactate elevation and hence, invariably has acidosis.
Defibrillation
After activating the emergency response system the lone rescuer should next retrieve an AED (if nearby and easily accessible) and then return to the victim to attach and use the AED. The rescuer should then provide high-quality CPR. When 2 or more rescuers are present, one rescuer should begin chest compressions while a second rescuer activates the emergency response system and gets the AED (or a manual defibrillator in most hospitals) (Class IIa, LOE C). The AED should be used as rapidly as possible and both rescuers should provide CPR with chest compressions and ventilations.
When any rescuer witnesses an out-of-hospital arrest and an AED is immediately available on-site, the rescuer should start CPR with chest compressions and use the AED as soon as possible. Healthcare providers who treat cardiac arrest in hospitals and other facilities with on-site AEDs or defibrillators should provide immediate CPR and should use the AED/defibrillator as soon as it is available. CPR should be performed while the defibrillator is readied. There is insufficient evidence to support or refute CPR for 2 mins before defibrillation.
When VF is present for more than a few minutes, the myocardium is depleted of oxygen and energy. A brief period of chest compressions can deliver oxygen and energy to the heart, increasing the likelihood that a shock will both eliminate VF (defibrillation) and be followed by ROSC. Before the publication of the 2005 AHA Guidelines for CPR and ECC, 2 studies suggested the potential benefit of CPR first rather than shock first. In both studies, although 1½ to 3 minutes of CPR before shock delivery did not improve overall survival from VF, the CPR-first strategy did improve survival among victims with VF if the EMS call-to-arrival interval was 4 to 5 minutes or longer. However, 2 subsequent randomized controlled trials found that CPR before attempted defibrillation by EMS personnel was not associated with a significant difference in survival to discharge. N Engl J Med. 2011 Sep 1;365(9):787-97.
Biphasic defibrillators are preferred because of the lower energy levels needed for effective cardioversion. We recommend that all defibrillations for patients in cardiac arrest be delivered at the highest available energy in adults (generally 360 J for a monophasic defibrillator and 200 J for a biphasic defibrillator).
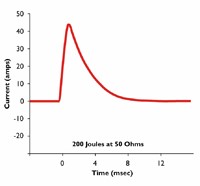
Monophasic Waveforms: A type of defibrillation waveform where a shock is delivered to the heart from one vector as shown below. In this waveform, there is no ability to adjust for patient impedance, and it is generally recommended that all monophasic defibrillators deliver 360J of energy in adult patients to insure maximum current is delivered in the face of an inability to detect patient impedance.

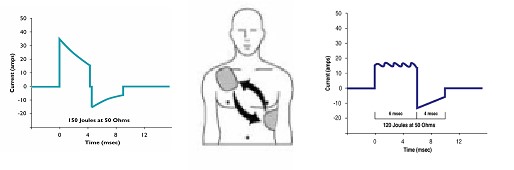
Biphasic Waveforms: A type of defibrillation waveform where a shock is delivered to the heart via two vectors. Biphasic waveforms were initially developed for use in implantable defibrillators and have since become the standard in external defibrillators.
While all biphasic waveforms have been shown to allow termination of VF at lower current than monophasic defibrillators, there are two types of waveforms used in external defibrillators. These are shown below.
Pulse Checks:
Therefore, pulse checks and rhythm analysis should only be performed during a planned interruption at the two minute interval following a complete cycle of cardiopulmonary resuscitation (CPR). Healthcare providers must not spend more than ten seconds checking for a pulse, and should start CPR immediately if no pulse is felt. The AHA 2015 Guidelines recommend that CPR be resumed for two minutes, without a pulse check, after any attempt at defibrillation, regardless of the resulting rhythm.
The lay rescuer should not check for a pulse and should assume that cardiac arrest is present if an adult suddenly collapses or an unresponsive victim is not breathing normally. The healthcare provider should take no more than 10 seconds to check for a pulse and, if the rescuer does not definitely feel a pulse within that time period, the rescuer should start chest compressions (Class IIa, LOE C).
Advanced Cardiac Life Support (ACLS)

Drug Therapy:
When VF/pulseless VT persists after at least 1 shock and a 2-minute CPR period, a vasopressor can be given with the primary goal of increasing myocardial blood flow during CPR and achieving ROSC. Epinephrine is currently used.
ACLS drug therapy during CPR is often associated with increased rates of ROSC and hospital admission but not increased rates of long-term survival with good neurologic outcome. Recent studies showed that epinephrine increased the chances of ROSC, but failed to improve long term survival.
Epinephrine
Epinephrine hydrochloride produces beneficial effects in patients during cardiac arrest, primarily because of its alpha-adrenergic receptor-stimulating (i.e., vasoconstrictor) properties. The alpha-adrenergic effects of epinephrine will increase afterload and can increase coronary perfusion pressure and cerebral perfusion pressure during CPR. The value and safety of the beta-adrenergic effects of epinephrine are controversial because they may increase myocardial work and reduce subendocardial perfusion. It may be reasonable to administer epinephrine as soon as feasible after the onset of cardiac arrest due to an initial nonshockable rhythm.
Vasopressin:
Vasoconstrictor which increases afterload, which increase diastolic pressure and increase coronary perfusion pressure and cerebral perfusion pressure. As per ACLS 2015 duidelines, Vasopressin does not offer any advantage over the use of epinephrine alone. N Engl J Med. 2008 Jul 3;359(1):21-30, Lancet. 2001 Jul 14;358(9276):105-9.Therefore, to simplify the algorithm, vasopressin has been removed from the 2015 ACLS Algorithm. However, the same guidelines contain a Class IIb recommendation to consider vasopressin for in-patient cardiac arrest. In another study, Vasopressin in combination with epinephrine demonstrated improved ROSC in cardiac arrest patients with initial arterial pH <7.2 compared with epinephrine alone. Ann Pharmacother. 2014 Aug;48(8):986-991. Also, it has to be noted that in none of the studies, was vasopressin inferior or has more adverse effects.
Antiarrythmics:
We suggest that antiarrhythmic drugs be considered after a second unsuccessful defibrillation attempt in anticipation of a third shock.
-
Amiodarone (300 mg IV with a repeat dose of 150 mg IV as indicated) may be administered in VF or pulseless VT unresponsive to defibrillation, CPR, and epinephrine.
-
Lidocaine (1 to 1.5 mg/kg IV, then 0.5 to 0.75 mg/kg every 5 to 10 minutes) may be used if amiodarone is unavailable.
-
Magnesium sulfate (2 g IV, followed by a maintenance infusion) may be used to treat polymorphic ventricular tachycardia consistent with torsade de pointes.
Steroids:
Steroids may provide some benefit when bundled with vasopressin and epinephrine in treating cardiac arrest. While routine use is not recommended , it would be reasonable to administer the bundle for inhospital cardiac arrest. JAMA. 2013 Jul 17;310(3):270-9 , Crit Care. 2014; 18(3): 308
End-Tidal CO2
End-tidal CO2 is the concentration of carbon dioxide in exhaled air at the end of expiration. Under normal conditions PETCO2 is in the range of 35 to 40 mm Hg. During untreated cardiac arrest CO2 continues to be produced in the body, but there is no CO2 delivery to the lungs. Under these conditions PETCO2 will approach zero with continued ventilation. With initiation of CPR, cardiac output is the major determinant of CO2 delivery to the lungs. If ventilation is relatively constant, PETCO2 correlates well with cardiac output during CPR.
The correlation between PETCO2 and cardiac output during CPR can be transiently altered by giving IV sodium bicarbonate. This is explained by the fact that the bicarbonate is converted to water and CO2, causing a transient increase in delivery of CO2 to the lungs. Therefore, a transient rise in PETCO2 after sodium bicarbonate therapy is expected and should not be misinterpreted as an improvement in quality of CPR or a sign of ROSC.
The correlation of PETCO2 with CPP during CPR can be altered by vasopressor therapy, especially at high doses (i.e. 1 mg of epinephrine).Vasopressors cause increased afterload, which will increase blood pressure and myocardial blood flow during CPR but will also decrease cardiac output. Therefore, a small decrease in PETCO2 after vasopressor therapy may occur but should not be misinterpreted as a decrease in CPR quality.
Persistently low PETCO2 values (<10 mm Hg) after 20 mins of CPR in intubated patients suggest that ROSC is unlikely.
Termination of resuscitative efforts — Determining when to stop resuscitation efforts in cardiac arrest patients is difficult, and little data exist to guide decision-making. Factors associated with poor and good outcomes are:
-
Duration of resuscitative effort >30 minutes without a sustained perfusing rhythm
-
Initial electrocardiographic rhythm of asystole
-
Prolonged interval between estimated time of arrest and initiation of resuscitation
-
Patient age and severity of comorbid disease
-
Absent brainstem reflexes
-
Normothermia
More objective endpoints of resuscitation have been proposed. Of these, the best predictor of outcome may be the end tidal CO2 level following 20 minutes of resuscitation. End tidal CO2 values are a function of CO2 production and venous return to the right heart and pulmonary circulation. A very low end tidal CO2 (<10 mmHg) following prolonged resuscitation (>20 minutes) is a sign of absent circulation and a strong predictor of acute mortality.
Asystole for 20 minutes is generally considered non-survivable.
Surviving to hospital discharge for in-house cardiac arrest is roughly 24% as per AHA, 2013 data.
References: 2015 AHA guidelines for BLS and ACLS
PEARLS:
-
Coronary angiography should be performed emergently (rather than later in the hospital stay or not at all) for cardiac patients with suspected cardiac etiology of arrest and ST elevation on ECG.
-
Studies of patients after cardiac arrest have found that a systolic blood pressure less than 90 mm Hg or a mean arterial pressure of less than 65 mm Hg is associated with higher mortality and diminished functional recovery ( 2015 ACLS guidelines).
-