Proportional Assist Ventilation
PAV is a spontaneous breathing mode that offers assistance to the patient in proportion to the patient’s effort. It can be considered as adaptive pressure support. In pressure support, the support is a fixed driving pressure. In PAV, the support is adaptive to keep work of breathing constant. In this mode, the magnitude of ventilator assistance (flow, volume or pressure) was neither predetermined nor constant but adjusted to the patient’s respiratory drive and mechanical obstacles to its output (i.e. Resistance and Elastance). If patient works harder, machine gives more support to decrease WOB. If patient is comfortable and not working hard, machine gives very little support. The drawback of this method is that if the patient is not working at all, the machine will not give any support. Hence, it is of no use in patients who doesn’t have any respiratory efforts and not spontaneously breathing.
It is a PC-CSV-adaptive mode of ventilation. It is also physiologically more close to spontaneous breathing compared with pressure support ventilation. Hence, patients would need less sedation.
Its main requirements are spontaneous breaths and intact neuromuscular drive. It avoids ventilator over-assistance and thereby prevents respiratory muscle disuse. It also reduces ventilator asynchrony and less sleep distortion. It can also be used as an alternate mode of non invasive ventilation.
PAV performs poorly in the presence of severe dynamic hyperinflation, Auto PEEP, expiratory flow limitation and respiratory muscle weakness.
How it works?
If the ventilator is to provide assistance in proportion to the patient’s effort, it needs to know how much effort the patient is making for each breath.
Flow and volume insertion into the lungs requires the exercise of a power, which, irrespective of its origin (inspiratory muscles, ventilator machine or both), can overcome the two main opposing forces: resistance of the respiratory system and elastance of the respiratory system.
According to equation of motion,
PTotal = Pvent + Pmus = Presistance + Pelastance + PEEPi
= Flow x Res + VT x Elastance + PEEPi
Pvent is also called Paw. Normal Pmus is between 5-10.
The pressure needed to ventilate the patient can be totally provided by the patient in spontaneously breathing patients, totally provided by the ventilator in controlled mechanical ventilation or shared between patient and ventilator. In other words, the total pressure required to ventilate is equal to tidal volume times Elastance plus flow times resistance. Hence, Ptotal equals patient’s generated muscular effort (Pmusc) plus ventilator generated pressure (Pvent).
Both PAV and NAVA are designed in a way that the pressure (i.e. work) to ventilate is shared between patient and ventilator in manner intended to maximize ventilator synchrony. Both PAV and NAVA respond to patient’s ventilatory demand by providing either proportional unloading of work of breathing or proportional unloading of electrical activity of diaphragm.
PAV+ instantaneously measures the flow and volume being pulled in by the patient, and, knowing the compliance and resistance of the respiratory system of the respiratory system, determines how much pressure to provide for each breath. Pressure needed by patient is proportional to instantaneous flow and volume.
All of today’s ventilators can easily measure flow and thus can calculate volume on a moment-to-moment basis. The calculation of respiratory system mechanics is performed automatically by the ventilator by applying, at random intervals of four to 10 breaths, a 300-ms pause maneuver at the end of selected inspirations. Then, it can calculate resistance, Elastance and compliance based on ventilator algorithms. The only variable in equation of motion that is not either directly measured or calculated is P total. Thus, the ventilator can calculate the pressure needed, at any given moment, to provide ventilation. If the clinician has set PAV at 60%, the ventilator would provide 60% of the calculated pressure, the remaining pressure being left to the patient to generate. That is, on a breath-to-breath basis the ventilator applies the calculated amount of pressure needed to meet the flow and volume demand of the patient based on the set PAV percentage, leaving the remaining work to the patient. Exhalation occurs when flow decreases to a preset level. Additionally, as the patient’s lung mechanics change, those ventilators that automatically measure R and E can adjust the amount of pressure needed to maintain the set PAV percentage. (Remember that the maximal pressure that ventilator can provide can’t exceed the alarm limit and minimum pressure that ventilator can provide is 4cm of H2O).
Specifically, PAV improves patient-ventilator synchrony during the onset of inspiration, by matching the patient’s inspiratory demand. That is, there is no limit to flow delivery, the ventilator responds to the patient’s demand up to the capabilities of the ventilator, regardless of the PAV setting. This differs from pressure ventilation, in which flow will decelerate when airway pressure meets the target level. In PAV there is no pressure target; pressure will increase, as will flow, as patient demand increases. Cycling is improved because the ventilator adjusts flow during the end of inspiration the same as it does during the onset. Thus, as patient effort starts to decrease, flow delivery decreases, and when flow decreases to the cycling criterion, the ventilator transitions to exhalation. However, triggering is not directly improved with PAV, compared to conventional ventilation. The patient still has to generate sufficient flow to trigger the ventilator.
Transition to expiration is also driven by Pmus. As the latter declines towards the end of neural inspiration, inspiratory flow gradually decreases and, when it reaches a preselected threshold, the ventilator terminates pressure generation. Thus, contrary to PSV and assist volume control (AVC), cycling off is determined by Pmus, minimizing expiratory asynchrony
Settings:
-
We set the proportion of assistance (generally between 10 and 90%) that we want the ventilator to provide, and the rest is up to the patient. i.e., if we set PAV at 80% assistance, that means that the ventilator will do 80% and the patient will do 20% of the work of breathing.
-
When selecting the appropriate %Support level, consider the following during initial setup and subsequent adjustments:
-
Wait a minimum of 10 to 15 breaths for the algorithm to stabilize the patient’s response to the new %Support setting before changing other settings.
-
Higher levels of support may prove uncomfortable to the patient, which may result in increased agitation. Be cautious when choosing %Support values higher than 80%.
-
Use the work of breathing (WOB) bar as a guide. Adjust the %Support setting to maintain the patient’s WOB within the “green” region. If the WOB Pt indicator is to the left or the right of the green region, the patient is being, respectively, over supported or under supported by the ventilator.
-
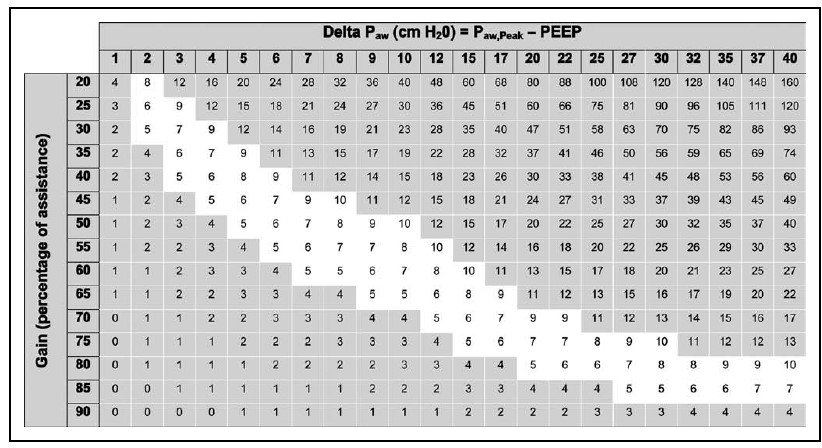
The Pmusc, estimated in cm H2O as (peak airway pressure – positive end-expiratory pressure) × [(100 – gain)/gain], was calculated from a grid at the bedside. The gain or % support is adjusted to keep Pmusc between 5 and 10 cm H2O.
-
Another method of adjusting % support is using the Delta PAW which is the difference of Ppeak and PEEP, where Ppeak is peak airway pressure. Once Delta PAW is known, the % support to be given to keep Pmusc in 5-10 range can be obtained from the table.
-
In other words, the set PAV % is the work provided by the ventilator
|
% Assist
|
Pt. Contribution
|
Proportionality
|
Amplification
|
|
25
|
75
|
1:3
|
1.3
|
|
50
|
50
|
1:1
|
2
|
|
75
|
25
|
3:1
|
4
|
|
90
|
10
|
9:1
|
10
|
- For PAV+ only, Esens represents the measured flow in L/min (not % of peak flow, as in Pressure Support breath types) at which the ventilator declares end of inspiration.
- In both PAV and NAVA, the clinician doesn’t set pressure, flow, volume or time. All of those variables are under complete control of patient. Essentially, ventilator proportionally unloads the patient’s effort.
- Ensure that correct ideal body weight, endotracheal tube size and maximum airway pressure (40 cmH2O) are entered correctly. Setting airway pressure limit is of paramount importance, since it will protect the lungs from over distension if run-away breaths occur.
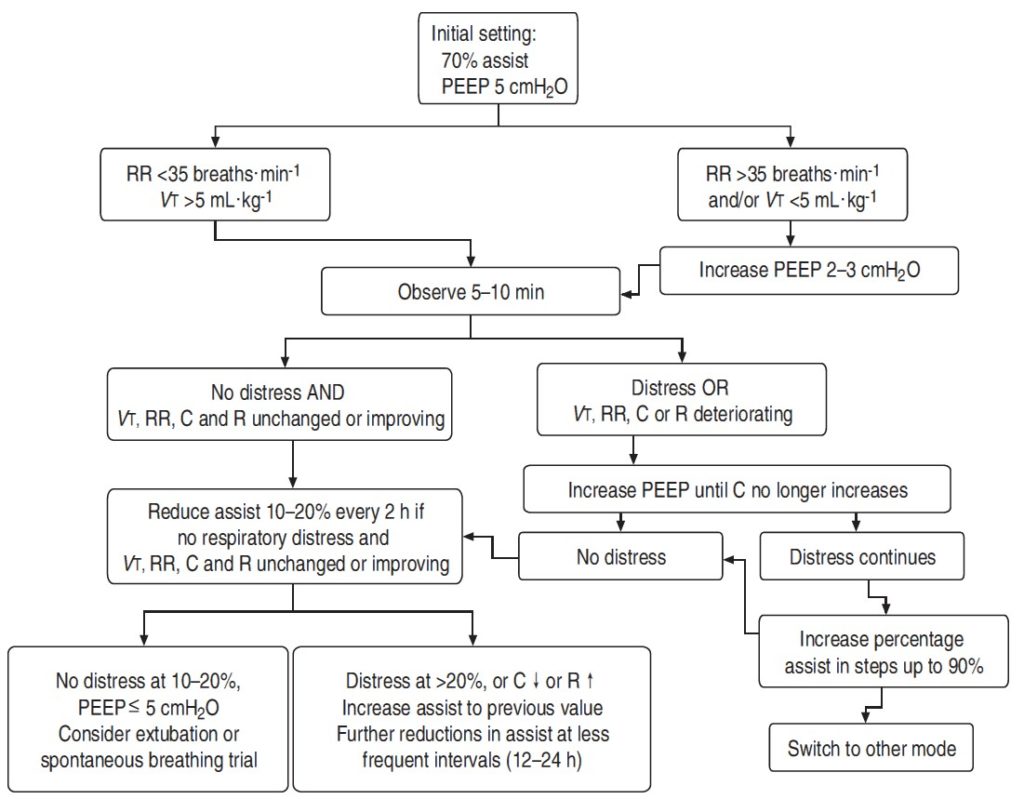
- Initial PEEP and inspiratory oxygen fraction (FiO2) are set using common criteria. The initial value of PEEP is set to 5 cmH2O. Also, subsequent hypoxaemia is managed as usual, by adjusting PEEP and Fio2. The response of compliance may be used to titrate PEEP; PEEP is increased until compliance no longer increases, signifying the end of recruitment.
- VT may be quite variable on PAV+. This is normal, partly reflecting the normal breath variability and partly events on previous modes (mainly over-assist). VT may be quite low (i.e. 3–4 mL/kg) and this is not uncommon. To the extent that respiratory rate does not increase concurrently and there are no other signs of distress, low VT is not an indication to change assist level.
- A high respiratory rate (even up to 50/min) need not by itself indicate distress. Other signs of distress should be present (e.g. sustained change in heart rate or blood pressure, accessory muscles use, sweating, etc.).
- PaCO2 may rise after switching to PAV+. Most commonly this is due to over-ventilation before PAV+. In these patients, central apneas upon switching to PAV+ may be observed. Be concerned only if the pH decreases below normal (i.e. 7.37). Acidemia without distress indicates depressed respiratory drive. These patients are not candidates for PAV+ until the cause of depressed drive is corrected.
- Very few patients continue to have distress at 70% of assist after adjusting PEEP. In these patients, increase percentage of assist in steps of 5% up to 90%. Wait 15–20 breaths between steps and observe for stretched out breaths (delayed cycling off or run-away). If stretched out breaths appear, decrease the assist to the previous level.
Drawbacks:
- PAV performs poorly in patients with severe dynamic hyperinflation, severe respiratory muscle weakness, poor respiratory drive and unconscious patients.
- Also, in PAV, higher peak flows may increase resistive workload with incomplete compensation as resistance measurements in current PAV models is not optimal.
- Because the assistance delivered during PAV+ is in proportion to the patient’s respiratory effort, patients with a high respiratory drive not related to the load per se (e.g., patients with metabolic acidosis or central nervous system diseases) may not be good candidates for PAV+, especially if the assistance is adjusted according to the respiratory effort.
PAV vs. Pressure Support:
In pressure support, the set pressure is fixed and may result in unnecessarily high assist resulting in respiratory muscle disuse and hyperventilation. This may lead to more sedation and weaning failure.
Also, in pressure support, since the driving pressure is fixed and if the patient wants high tidal volumes, he has to put more effort and may get fatigued easily. In PAV, even if he wants more volumes, the ventilator will increase the driving pressure in proportion to patient efforts.
PAV provides better matching between effort and tidal volume. Hence, it preserves respiratory muscle strength and facilitates weaning.
In a trial, PAV is associated with better ventilator synchrony and faster weaning from ventilator when compared to pressure support ventilation.
Even though PAV improved ventilator synchrony compared with PS, it didn’t improve sleep quality in COPD patients. In other studies, PAV was shown to improve sleep quality.
PEARLS:
-
In pressure control modes, the Pvent is kept constant and Pmusc can change. However, in PAV, the ventilator calculated Ptotal and shares it between Pmusc and Pvent.
-
Thanks for giving us so useful information. Very practical and feasible. How can I include your post as a reference?
I am glad it was useful
Very informative! thank you!
For a prolonged ventilator course, would you initially use PAV in 2- h hour”trials” as we do with PS trials?